Sleep and Anxiety: How to Break the Insomnia Loop
Anxiety keeps you awake. Then poor sleep makes anxiety worse the next day. Then the fear of another bad night turns bedtime itself into a threat. This loop has a name, a mechanism, and a set of techniques that break it.
Key Insight: CBT-I resolves chronic insomnia in 70-80% of cases and outperforms sleeping pills long-term. The core mechanism — stimulus control and sleep restriction — breaks the conditioned anxiety between your brain and your bed.
The Anxiety-Insomnia Loop
Anxiety and insomnia do not sit side by side — they feed each other. The loop usually starts with a stressful period: a new job, a breakup, a health scare, a deadline. You lose a few nights of sleep. That is normal. What makes it chronic is what happens next.
After a week of bad nights, your brain begins to associate the bed itself with not sleeping. You start checking the clock. You start worrying about tomorrow as you try to fall asleep. The worry produces sympathetic arousal — elevated heart rate, shallow breathing, racing thoughts — which is physiologically incompatible with sleep onset. The harder you try, the more awake you become.
This is the hyperarousal model of insomnia, developed by sleep researchers in the 1990s and 2000s. People with chronic insomnia are not just tired during the day; they are measurably more aroused — higher cortisol, higher metabolic rate, higher heart rate — around the clock. Their stress system is stuck in the on position, and the bedroom becomes the place where that arousal peaks.
The Loop in Four Steps
Why Your Brain Treats Bed Like a Threat
The mechanism behind chronic insomnia is classical conditioning — the same process Pavlov described. A neutral stimulus (the bed) gets paired repeatedly with an unpleasant state (lying awake, frustrated, anxious). After enough pairings, the stimulus alone produces the state. Your bed becomes an anxiety trigger.
If you have ever felt relaxed on the couch at 10 PM, then wide awake the moment you get into bed, you have experienced this directly. Your body is not being irrational. It has learned that the bed means arousal, so it delivers arousal on cue.
The problem is reinforced by what sleep researchers call the 20-minute rule violation. When people cannot sleep, they stay in bed hoping sleep will come. That is the single most damaging thing you can do. Every minute of frustrated wakefulness in bed strengthens the bed-anxiety association. You are actively training your brain to fail at sleep.
Operant conditioning also plays a role. Checking your phone while lying awake temporarily relieves boredom — that relief rewards the wakefulness. Getting out of bed to eat something, scroll, or watch TV turns your bed into a place where nothing much happens except worry. Eventually, you associate the bed with planning tomorrow, replaying today, or simply staring at the ceiling.
What Actually Works: CBT-I
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment recommended by the American Academy of Sleep Medicine and the American College of Physicians. It is more effective than sleeping pills for chronic insomnia, and unlike medication, its benefits persist after treatment ends.
A 2015 meta-analysis published in the Annals of Internal Medicine reviewed 20 randomized trials of CBT-I and found consistent improvements across every metric: faster sleep onset, fewer wakings, longer total sleep time, higher sleep efficiency. The effects held up at 6- and 12-month follow-ups. For a non-pharmacological treatment, those are exceptional results.
The standard protocol runs 4 to 8 sessions. It has four components: stimulus control, sleep restriction, cognitive therapy, and sleep hygiene education. The first two do most of the heavy lifting. The cognitive work helps you stop catastrophizing about bad nights. Sleep hygiene, despite being the most popular piece of advice online, is actually the smallest contributor to the treatment effect.
CBT-I vs Sleeping Pills
A landmark JAMA trial (Morin et al., 2009) found CBT-I outperformed pharmacotherapy at 6 months. The combination of both was no better than CBT-I alone for long-term outcomes.
Response Rate
Roughly 70 to 80 percent of patients with chronic insomnia show clinically meaningful improvement. Around half achieve full remission.
Stimulus Control and Sleep Restriction
These are the two most powerful techniques in CBT-I. They work by directly unlearning the bed-anxiety association.
Stimulus control re-teaches your brain that the bed is for sleep. The rules are simple and strict: only get into bed when sleepy, use the bed only for sleep and intimacy, get out of bed if you are awake for more than 20 minutes, keep a fixed wake time regardless of how you slept, and avoid daytime naps. The goal is to rebuild the association: bed equals sleep, nothing else.
Sleep restriction, developed by Spielman and colleagues in 1987, sounds counterintuitive but works exceptionally well. You deliberately shrink the time you spend in bed to match the time you actually sleep. If you are sleeping 5.5 hours but spending 8 hours in bed, you restrict your time in bed to 5.5 hours. This produces mild sleep deprivation, which builds sleep pressure and makes it much harder to lie awake. Once your sleep efficiency rises above 85 to 90 percent, you gradually extend your time in bed.
The first week of sleep restriction is hard. You will feel more tired. But within two to three weeks, most people find they fall asleep quickly, stay asleep, and wake feeling rested. The key measurement is sleep efficiency — the ratio of time asleep to time in bed. Raising it to 90 percent or higher is the signal that the bed-sleep association is rebuilding.
What to Do at 3 AM
The single most important moment in breaking the insomnia loop is what you do when you wake up in the middle of the night and cannot get back to sleep. Most people stay in bed, check the time, scroll their phone, and spiral. Every one of those choices strengthens the loop.
The 3 AM Protocol
- Get out of bed.If you have been awake for 20 minutes or you feel frustration building, leave the bedroom. The rule is not about precise minutes — it is about the feeling.
- Go somewhere dim.Use the lowest light possible. A book light, a candle, a red-tinted lamp. Bright light at 3 AM shifts your circadian rhythm and makes tomorrow worse.
- Do something dull.Read something slightly boring. Fold laundry. The goal is a low-stimulation activity that lets sleepiness return. No puzzles, no shows with cliffhangers, no work.
- Do not look at the clock.Every clock-check triggers math: "If I fall asleep now I will get 4 hours." That math triggers anxiety. Turn the clock away. Cover the microwave.
- No scrolling.The content rabbit holes of social media and news produce dopamine and emotional activation — both antagonistic to sleep. A paper book at dim light is the gold standard.
- Return when sleepy.Only get back into bed when you feel actual sleepiness — eyelids heavy, attention drifting. If sleep does not come in another 20 minutes, get out again.
How Reverie Supports the Process
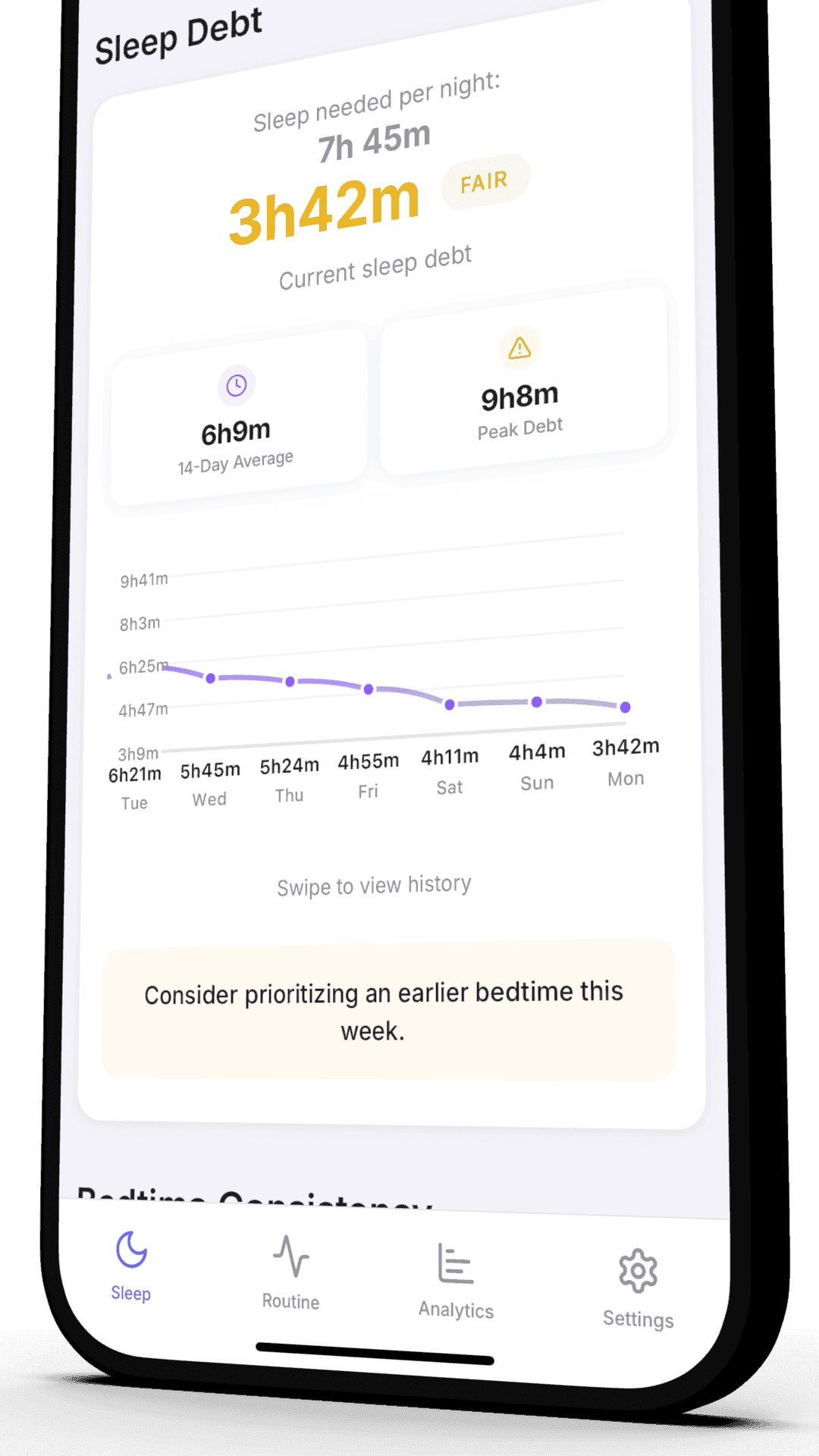
CBT-I is not a single-night fix. It is a multi-week process in which you track specific metrics, watch them trend, and confirm that the loop is loosening. The metric that matters most is sleep onset latency — how long it takes you to fall asleep after getting into bed. In someone with anxiety-driven insomnia, this number starts high (often 45 minutes or more) and drops as the association between bed and arousal weakens.
Reverie reads your Apple Watch data to estimate sleep latency night by night. You can see the trend across weeks, which is the feedback loop that keeps you consistent. When your latency drops below 20 minutes and sleep efficiency rises above 85 percent, you know the protocol is working.
What Reverie Tracks for CBT-I Progress
- • Sleep onset latency trend across 30 and 90 days
- • Sleep efficiency percentage night by night
- • Total time in bed vs total time asleep
- • Number of nighttime awakenings and their duration
- • Consistency of wake time, which is the backbone of the protocol
Reverie is not a therapist and does not replace one. If your insomnia has lasted more than three months, is disrupting work or relationships, or is paired with panic, a trained CBT-I practitioner is worth the investment. Tracking gives you and your therapist a shared view of what is actually happening.
References
- Trauer JM, Qian MY, Doyle JS, Rajaratnam SM, Cunnington D. "Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis." Ann Intern Med. 2015;163(3):191-204. Source
- Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. "Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians." Ann Intern Med. 2016;165(2):125-133. Source
- Riemann D, et al. "The hyperarousal model of insomnia: a review of the concept and its evidence." Sleep Med Rev. 2010;14(1):19-31. Source
- Morin CM, et al. "Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial." JAMA. 2009;301(19):2005-2015. Source
- Spielman AJ, Saskin P, Thorpy MJ. "Treatment of chronic insomnia by restriction of time in bed." Sleep. 1987;10(1):45-56. Source
Related Articles
Sleep Efficiency Explained
The single metric that tells you whether CBT-I is working. How to measure it and raise it above 90 percent.
Melatonin Supplements: What the Evidence Says
Why melatonin is not a sleeping pill, and the narrow cases where it genuinely helps with anxiety-driven insomnia.
Track Your Path Out of Insomnia
Join our beta program and measure your sleep latency, efficiency, and consistency night by night. Reverie turns your Apple Watch data into the feedback loop CBT-I needs to work.
Free beta access. Shape the product. First to get updates. Requires Apple Watch.
Written by the Reverie Team
Based on sleep research and scientific studies